When the “Protective” Position Isn’t Protective: A Counterintuitive Observation in Rotator Cuff Tendinopathy

A single-patient observation suggests that muscle–tendon length may influence shoulder pain more than we assume.
A Counterintuitive Patient Response
A patient’s answer to a simple question about her shoulder pain stopped me in my tracks.
When I asked what eased the pain, she replied:
“When I position my arm above my head, it feels better.”

That response seemed counterintuitive. Most patients with shoulder pain instinctively keep their arm close to the body—often in a sling-like posture—to avoid discomfort.
Yet in this case, the opposite position provided relief.
Why This Matters
Rotator cuff–related shoulder pain is one of the most common musculoskeletal conditions seen in clinical practice. Clinicians often recommend protective positions that keep the arm close to the body and limit movement.
But what if some of these positions increase tendon strain rather than reduce it?
This patient encounter prompted me to reconsider how muscle–tendon length and resting position might influence symptoms in rotator cuff tendinopathy.
The Clinical Encounter
I asked the patient to demonstrate the position she used for pain relief. Using her non-painful arm, she lifted the painful arm and placed the forearm on top of her head.
My immediate reaction was skepticism. Positioning the arm above the head to relieve shoulder pain did not seem to make sense.
I considered whether the symptoms might originate from the cervical spine. The shoulder abduction test (Bakody’s sign) is commonly used to detect arm pain caused by cervical nerve root compression.
However, isolated neck movements did not provoke or relieve her shoulder pain. This finding suggested that the Bakody-like response was unlikely to originate from the cervical spine.
As the plan of care progressed, the patient’s history and physical examination pointed toward a working diagnosis of rotator cuff syndrome, a form of shoulder tendinopathy.
Subsequent imaging supported this hypothesis. A shoulder MRI revealed:
- Moderate fraying and thinning of the supraspinatus tendon
- Mild fraying and thinning of the infraspinatus tendon
The supraspinatus and infraspinatus are two of the four muscles that make up the rotator cuff. The other two are the teres minor and the subscapularis. Together, these muscles stabilize the shoulder joint and allow the arm to lift and rotate.
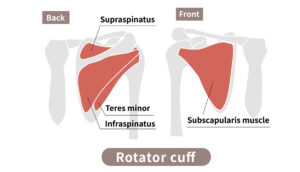
Caption of Teres minor is an error, it should be Teres major
Of these four tendons, the supraspinatus most commonly develops tendinopathy.
Working Hypothesis
Tendon symptoms are strongly influenced by mechanical loading, including both compressive and tensile forces.
The strain placed on a tendon changes as the muscle–tendon unit lengthens or shortens.
A possible explanation for this patient’s experience is:
- Shorter muscle–tendon length → less strain → less pain
- Longer muscle–tendon length → greater strain → more pain
This framework may help explain why certain arm positions reduce symptoms while others provoke them.
Tendon Length & Arm Position
The following table illustrates how different arm positions may place rotator cuff tendons at either longer or shorter resting lengths.
| Tendon | Position where the muscle–tendon unit is at its longest length (potentially more painful) | Position where the muscle–tendon unit is at its shortest length (potentially less painful) |
| Supraspinatus | Hand in the back pocket of pants (internal rotation, adduction) | Arm or forearm resting on top of the head or hand behind the head (external rotation, abduction) |
| Infraspinatus | Arm reaching toward the opposite armpit or positioned in a sling (internal rotation, adduction) | Arm or forearm resting on top of the head or hand behind the head (external rotation) |
| Subscapularis | Arm above the head or hand behind the head (external rotation, abduction) | Hand positioned in the back pocket of pants (internal rotation, adduction) |
| Teres Minor | Arm across the body with hand in the opposite armpit (internal rotation, adduction, extension) | Arm or forearm resting on top of the head or hand behind the head (external rotation, abduction) |
What This Observation Suggests
This is a single-subject clinical observation, not a definitive conclusion.
However, it raises an interesting question:
Could resting muscle–tendon length influence symptoms in rotator cuff tendinopathy?
Answering this question would require a systematic study in a larger group of patients with confirmed tendinopathy.
Implications for Rehabilitation
This concept may also help guide rehabilitation strategies, particularly when prescribing isometric strengthening exercises.
Individuals can perform isometric exercises at different muscle–tendon lengths to allow gradual tendon adaptation.
Progressively training the muscle–tendon unit across different lengths allows the tissues to adjust to increasing mechanical demands. Starting at shorter lengths may reduce strain and pain, while gradually progressing toward longer lengths prepares the tendon for functional loading.
Clinical Takeaway
When treating rotator cuff–related shoulder pain, clinicians often assume that keeping the arm close to the body will reduce symptoms.
However, this position places the shoulder in internal rotation and adduction, which may increase tensile loading on the supraspinatus and infraspinatus tendons.
Potential position to ease the pain of the subscapularis muscle. Potential position to provoke pain of Surpraspinatus, Infraspinatus, Teres Major
In some patients, positioning the arm above the head or in external rotation may reduce tendon strain by placing certain rotator cuff tendons at a shorter resting length.


The key lesson is simple:
The position that looks most protective is not always the position that unloads the tendon.
Instead, patients & clinicians should:
- Observe the positions naturally adopted for relief
- Consider how muscle–tendon length influences tendon strain
- Use these observations to guide resting positions and exercise progression
Sometimes patients reveal biomechanical solutions before we fully understand them
The information on this website is not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment. You are encouraged to perform additional research regarding any information available through this website, with other sources, and consult with your physician