Lateral Pelvic Tilt Sitting
When oriented normally, the pelvis appears level and symmetrical. But in individuals with a lateral pelvic tilt (also called pelvic obliquity), one side of the pelvis appears lower than the other side.
Lateral pelvic tilt can both cause and compensation to avoid musculoskeletal pain. It can be a contributing factor to jaw pain, headaches, shoulder, back, and/or buttock/hamstring pain primarily occurring on one side of the body. Conversely lateral pelvic tilt may occur as an automatic compensation to avoid musculoskeletal pain.
Lateral pelvic tilt is considered a deviation from normal and has many possible causes: spinal scoliosis; limited hip joint motion; small hemi-pelvis; atrophy of gluteal muscles; structural anatomical hip joint variations; anatomical or functional leg length discrepancy; and lopsided chair seat. But since it also can help prevent pain, it presents a conundrum: should it be treated or not?
Lateral pelvic tilt is commonly assessed in standing and less frequently assessed when sitting. When standing the legs can influence the lateral pelvic tilt; when sitting the influence of the legs is minimized. This article will focus on lateral pelvic tilt when sitting.
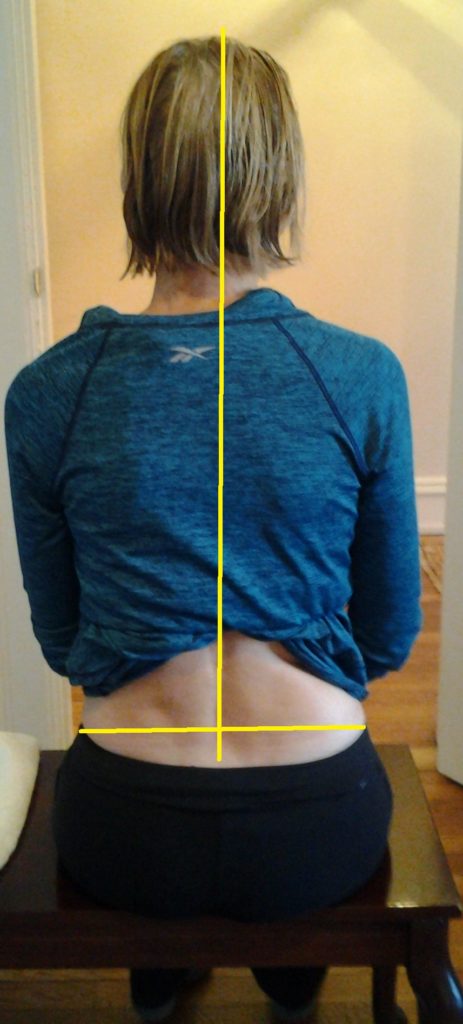
In the figure above, the left pelvic bone is lower than the right, and the center of mass is shifted to the left. This illustrates lateral pelvic tilt sitting.
Many individuals will spend more time sitting then standing or walking, looking at computer screen, commuting, and participating in recreation. Some individuals could be described as sitting ultra-marathoners. This repetitive use functional activity may contribute to musculoskeletal pain associated with lateral pelvic tilt sitting.
In order to determine if lateral pelvic tilt sitting is contributing to pain or compensating for pain requires problem solving and critical thinking.
Anatomical lateral pelvic tilt: a boney structural deviation is considered an anatomical (structural) lateral pelvic tilt, and could include hip joint dysplasia, scoliosis, and/or a small hemipelvis meaning that one half of the pelvis is smaller than the other half. An anatomical lateral pelvic tilt is not likely to change, so the patient needs adaptations or accommodations.
Functional lateral pelvic tilt: occurs in response to repetitive functional movements, sustained alignments which induce changes in muscular length and muscular imbalance.
When we sit with legs crossed it results in asymmetrical biomechanical changes, due to the different forces on the top and bottom legs. The majority of individuals cross right leg over left with greater frequency then left leg over right. This can alter muscle length and alignment in the following ways:
- Curve of lumbar spine (right lumbar concavity)
- Lumbar pelvic region rotating to the right
- Increase in pressure on the left hip joint/gluteal muscles
- The top right leg will be in habitual position of hip flexion, adduction, lateral femoral rotation
- The bottom left leg will be in habitual position of hip flexion, adduction, and medial femoral rotation
How to problem solve whether sitting in lateral pelvic tilt contributes to pain or avoids pain:
Sit on a firm flat surface with feet touching ground. Put a ¼” lift such as a magazine under the sit bone on one side of pelvis.
First put the lift under the sit bone of the lower side of the pelvis. Do you feel more balanced or less balanced? Do you feel more pain, less pain, or no change? Have a friend take a photo as in above figure to discern whether pelvis is level, and whether the trunk is centered over the pelvis.
Next, put the lift under the sit bone on the higher side of the pelvis, and consider the same questions: Do you feel more balanced or less balanced? Do you feel more pain, less pain, or no change? Have a friend take another photo to discern whether pelvis is level, and whether the trunk is centered over the pelvis.
Switch back and forth between no lift, lift under low side, lift under high side to observe for consistent changes in degree of perceived balance, pain, and orientation of pelvis and trunk.
Because there are 3 parameters (pain, balance, and orientation) it can be challenging to sort out the most optimal response. It is unlikely that a simple butt lift will solve the multifaceted problem, though it can be one simple intervention to help. A physical therapist can help sort out the best intervention.
Damien Howell Physical Therapy – 804-647-9499 – Fax: 866-879-8591 At-Home, At Office, At Fitness Facility – I come to you, I do home visits Damien@damienhowellpt.com