Downsides of steroid injections for hip pain – What 3 patients taught me
Three patients with chronic hip pain prompted me to dive deeper into the effectiveness and risks of the common intervention of corticosteroid injection for musculoskeletal pain syndromes.
Patient A complains of difficulty lifting his leg to put his pants on when standing and difficulty lifting his leg to transfer into his car. He had a total hip replacement. Years later, he was treated for a rare occurrence of impingement of the iliopsoas tendon with an injection using fluoroscopy (X-ray). He participated in a full round of physical therapy following the injection. Unfortunately, he reports no progress in improving his ability to lift his leg during functional activities.
Patient B complains of discomfort and weakness in the left hip. After standing more than 10 to 15 minutes and/or walking, he experiences weakness and a lack of control of the leg. He has a history of many years of symptoms, multiple interventions (extensive physical therapy, multiple surgeries), and multiple corticosteroid injections. Despite extensive Physical Therapy, strengthening exercises, movement pattern training, and progressive ambulation, the weak symptoms persist.
Patient C complains of hip and buttock pain when standing or walking for brief periods, such as standing to prepare meals and during exercise walking. It has been present for 10 years and has been diagnosed with “hip spine syndrome”. She has had 12 injections in the back and hip region for diagnostic and intervention over the last 4 years. Despite Physical Therapy, strengthening exercises, movement pattern training, and progressive ambulation, the weak symptoms persist.
These cases have less than satisfactory outcomes. The common intervention is corticosteroid injections.
These cases prompted me to review and investigate the benefits and risks of injections for musculoskeletal problems.
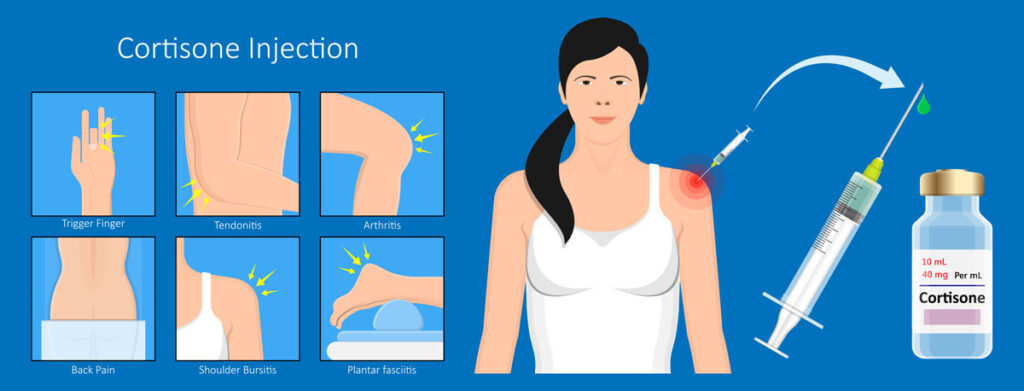
There are several different types of injections for hip pain that may be offered for several reasons. Injections can be intra-articular (injected into the joint), or extra-articular. Injections (outside the joint). Injections are aimed at tendons, bursa, or nerves. The material injected is corticosteroid, or anesthetic, or both. The injection uses either an anatomical landmark or blind or under imaging (X-ray or ultrasound) to reach the target tissue.
The purpose is to aid in diagnosis or reduce inflammation, pain, and disability.
My review of literature shows at the present time limited evidence, conflicting evidence, no clear consensus on the optimal method for the use of injections for painful musculoskeletal hip problems. [1]
The following is my attempt to use a dialectic process to tackle the uncertainties and questions associated with injections for hip pain.

PT & Exercise First? or Injection First?
Question: Does it make a difference whether the first intervention is an injection or Physical Therapy exercise?
Thesis: An injection can provide rapid pain reduction, enabling a patient to participate more fully and effectively in exercise, which can address the underlying problem.
Antithesis: B.K. Coombes and colleagues in a well-designed study of 165 individuals with chronic lateral elbow pain found that using corticosteroid with local anesthetic, anatomical landmark blind injection in combination with Physical Therapy and exercise did not support the practice of using injection to facilitate active rehabilitation exercise. The recurrence rate was higher in individuals receiving blinded steroid injection compared to placebo. It was found that the combination of blinded steroid injections in combination with Physical Therapy and exercise had no beneficial effect on recovery or recurrence. However, in the absence of blinded steroid injection, Physical Therapy and exercise provided short-term benefits as well lowest reoccurrence and complete recovery at 1 year. [2]
Patient A received an injection first then Physical Therapy and exercise.
Synthesis: The short-term benefits of steroid injection combined with Physical Therapy exercise management for Patient A may have been influenced by the possibility of masking of symptoms and inhibition of tissue healing. Movement pattern training works best if pain symptoms are available to provide feedback in efforts to learn to move in a more optimal manner.
Begin physical therapy and exercise management before considering injections for musculoskeletal pain syndromes.
Injection by anatomical landmarks blind vs injection guided by imaging
Question: Does it make a difference whether the injection technique uses an anatomical landmark (blind) vs under imaging?
Thesis: The advantages of landmark-guided (blind) steroid injections are that they are cost-effective, time-efficient, and easily performed in the clinical setting. [3]
Antithesis: There are multiple bursae at multiple locations; some are native bursae, and some are acquired bursae. Acquired bursae develop in response to friction that occurs between tendons and bony prominences. A blind injection may miss the inflamed bursa, and the medication may spread to adjacent tendinous tissue.
Potential side effects of steroid injections include muscle atrophy, tendon rupture, and accelerated progression of osteoarthritis. [4] Steroids and anesthetics can have a cytotoxic effect, inhibiting healing, masking pain,and making monitoring therapeutic exercise more challenging. [5]
Patient Be is an example of persistent hip weakness correlating with multiple anatomical landmark blind steroid injections.
Synthesis: The risks of missing the inflamed tissue, inhibiting tissue repair, and unintended adverse effects on muscle tissue associated with anatomical landmark blind injection outweigh the benefits of cost-effective, time-efficient treatment of blind injections. Using image-guided extra-articular injections increases likely hood of hitting the target tissue, thereby facilitating potential benefits.
Injections should employ methods that allow visualization of medication delivery.
Cortisone Injection - Risks & Side Effects
Question: What are the risks of injections?
Thesis: Extra-articular corticosteroid injections are widely used for a diverse musculoskeletal problems and are generally considered safe.
Antithesis: Extra-articular corticosteroid injections can cause muscular atrophy as a side effect, ranging from localized weakness to more widespread, drug-induced myopathy. [4]
S. Pace and colleagues observed that extra-articular corticosteroid injections can lead to muscle atrophy and strength loss. These side effects, which the medical community often overlooks, usually appear 2–4 months post-injection but can be late by as much as a year. [6]
jiHwan Lee and colleagues examined the influence of frequent corticosteroid injections of rotator cuff muscles (shoulder), finding adverse effects on the genes and muscle proteins contributing to muscle atrophy (weakness), inflammation, and tissue fibrosis. [7]
Patient C is an example of overutilization of injections. It reminds me of humorist Will Rogers saying, “If you find yourself in a hole, stop digging.”
If you find yourself in a hole ,stop digging
Synthesis: The recommendation by K. Zhang and colleagues regarding intra-articular corticosteroid injections is to use the lowest possible concentration and exposure. [5] This recommendation is applicable to extra-articular injection as well.
Injections should be used at the lowest possible concentrations & exposure.
Summation:
Thesis: Corticosteroid injections offer significant, rapid, short-term relief for hip pain
Antithesis: Corticosteroid injections carry risks and offer little long-term benefit
Synthesis:
- Begin physical therapy and exercise management before considering injections for musculoskeletal pain syndromes.
- Injections should employ methods that allow visualization of medication delivery.
- Injections should be used at the lowest possible concentrations & exposure.
References:
- Benzon HT, Elmofty D, Shankar H, et al. Use of corticosteroids for adult chronic pain interventions: sympathetic and peripheral nerve blocks, trigger point injections - guidelines from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, the American Society of Interventional Pain Physicians, and the International Pain and Spine Intervention Society. Reg Anesth Pain Med 2025 doi: 10.1136/rapm-2024-105593 [published Online First: 20250312].
- Coombes BK, Bisset L, Brooks P, Khan A, Vicenzino B. Effect of corticosteroid injection, physiotherapy, or both on clinical outcomes in patients with unilateral lateral epicondylalgia: a randomized controlled trial. JAMA 2013;309(5):461–9 doi: 10.1001/jama.2013.129.
- Saha P, Smith M, Hasan K. Accuracy of Intraarticular Injections: Blind vs. Image Guided Techniques-A Review of Literature. J Funct Morphol Kinesiol 2023;8(3) doi: 10.3390/jfmk8030093 [published Online First: 20230629].
- Kamel SI, Rosas HG, Gorbachova T. Local and Systemic Side Effects of Corticosteroid Injections for Musculoskeletal Indications. AJR Am J Roentgenol 2024;222(3):e2330458 doi: 10.2214/AJR.23.30458 [published Online First: 20231220].
- Zhang K, Li M, Yao W, Wan L. Cytotoxicity of Local Anesthetics on Bone, Joint, and Muscle Tissues: A Narrative Review of the Current Literature. J Pain Res 2023;16:611–21 doi: 10.2147/JPR.S398329 [published Online First: 20230227].
- Pace CS, Blanchet NP, Isaacs JE. Soft Tissue Atrophy Related to Corticosteroid Injection: Review of the Literature and Implications for Hand Surgeons. J Hand Surg Am 2018;43(6):558–63 doi: 10.1016/j.jhsa.2018.03.004 [published Online First: 20180403].
- Lee J, Lho T, Lee J, Lee J, Chung SW. Influence of Frequent Corticosteroid Local Injections on the Expression of Genes and Proteins Related to Fatty Infiltration, Muscle Atrophy, Inflammation, and Fibrosis in Patients With Chronic Rotator Cuff Tears: A Pilot Study. Orthop J Sports Med 2024;12(6):23259671241252421 doi: 10.1177/23259671241252421 [published Online First: 20240603].
The information on this website is not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment. You are encouraged to perform additional research regarding any information available through this website, with other sources, and consult with your physician