Foot Pain – Lifestyle Changes

After assisting a patient with several musculoskeletal concerns over the years, I received a new request that helped me recognize a recurring pattern among similar requests from other patients.
He was requesting assistance in obtaining custom orthotic shoe inserts for foot pain. Shoe orthotics is an intervention that, over the years, I have developed an expertise in.
I asked what he thought might have triggered the recent increase in foot pain, including whether any changes in activity or exercise could be placing additional stress on his feet. He explained that he had recently retired and was now spending more time at home.
Another patient requested custom orthotics to help relieve bunion pain, which has been getting worse. Over the previous several months. She has noticed the big toe is starting to cross over the second toe. During the Physical Therapy home visit, I observed a tray near the front door filled with shoes, which suggested that she routinely removed her shoes upon entering the house.

During the COVID-19 pandemic, I noticed more patients contacting me about new-onset foot pain. Stuck at home, we were spending less time wearing shoes.
I also notice a seasonal pattern. During Richmond summers, many people spend more time barefoot while vacationing at the river, bay, or beach. Bulent Alvanak et.al. used a search of Google Trends data for “Plantar Fasciitis” from 2004 to 2024 and found interest peaked in the summer and declined in winter. (Alyanak & Bagcier, 2026)

These recurring presentations prompted me to ask whether the issue was less about needing more support and more about spending fewer hours wearing supportive footwear and being barefoot.
Thesis:
Many patients assume that custom orthotics or over-the-counter arch supports are the best solution for their foot pain.
The common history is a temporal relationship with the onset of symptoms and an increased amount of time going barefoot.
Going barefoot is unlikely to be the sole cause of foot pain. Rather, it may represent one component of a broader change in mechanical loading."
Antithesis:
Natalie Collins and colleagues conducted a meta-analysis and concluded that, for individuals with lower-limb overuse injuries, the evidence base for orthotic use is generally too limited and low quality to clearly support or refute their effectiveness. (Collins et al., 2007)
The review also found no meaningful difference between custom and prefabricated foot orthotics, suggesting that either custom or over-the-counter options may be reasonable depending on the patient’s needs, preferences, and response to treatment.
Synthesis:
Orthotics only influence foot mechanics while they are being worn. If patients spend much of the day barefoot, even a well-designed orthotic has limited opportunity to affect cumulative tissue loading.
A very bright Physical Therapy colleague of my who is an expert on orthotics says, “The best orthotic is the one that a patient will wear.” If you spend a lot of time barefoot you are not wearing the orthotic.
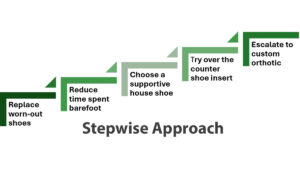
A Stepwise Approach:
Start with “shoe therapy” before moving to orthotics. This approach emphasizes improving the footwear environment first, then escalating only if symptoms persist.
- Replace worn-out shoes. Shoes that have lost cushioning, structure, or support may contribute to ongoing foot pain and should be replaced before adding an insert.
- Reduce time spent barefoot. Avoid or minimize barefoot activity when possible. If shoes are removed for cultural, religious, or household reasons, consider supportive indoor footwear that respects those needs. If you have already purchased orthotics, decide to wear them consistently at home.
- Choose a supportive house shoe. Select an indoor shoe or sandal that is easy to put on and take off, has a contoured footbed, and provides some lateral support, such as a heel strap.

- Try an over-the-counter insert if shoe therapy is not enough. If symptoms continue despite better footwear habits, consider starting with a prefabricated shoe insert. Monitor your response over time to determine whether it provides adequate relief.
- Escalate to custom orthotics when appropriate. If an over-the-counter insert does not provide sufficient improvement, then a custom orthotic may be considered—ideally one that can be worn consistently in a supportive house shoe.
Patients often seek the treatment they believe they need. Clinicians and patients, however, should first ask what changed before symptoms began. Identifying changes in activity, footwear, and lifestyle may reveal modifiable contributors that are more important than selecting the 'right' orthotic. Minimize barefoot time to alter cumulative tissue loading with principles of load management.
Reference:
Alyanak, B., & Bagcier, F. (2026). From Pain to Search: Mapping USA and Global Interest in Plantar Fasciitis. J Am Podiatr Med Assoc, 116(3). https://doi.org/10.3390/japma116030026
Collins, N., Bisset, L., McPoil, T., & Vicenzino, B. (2007). Foot orthoses in lower limb overuse conditions: a systematic review and meta-analysis. Foot Ankle Int, 28(3), 396–412. https://doi.org/10.3113/FAI.2007.0396
The information on this website is not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment. You are encouraged to perform additional research regarding any information available through this website, with other sources, and consult with your physician