Heel Whip When Running
There is a growing body of evidence among healthcare professionals to suggest the way we run contributes to the risk of a repetitive use injury, and that gait retraining is an effective intervention for managing repetitive use injuries. There is less consensus and much debate on which movement faults are more important. Common movements that can be easily observed with slow motion video analysis are: foot strike pattern, knee flexion during stance, hip extension during stance, trunk lean, stride length, vertical displacement of center of mass (up and down motion), rate of impact loading (sound), and pronation. Each of these have been linked to the development of repetitive use injuries.
Recent work by Richard Souza of University of California San Francisco identified an interesting movement fault not commonly recognized which may be of importance; he describes it as “heel whip”. Heel whip is a medial (inward) or lateral (outward) rotation of the foot (heel) relative to the midline of the body occurring when the foot comes off the ground AND is best observed from behind the runner. If you are self-assessing whether you have an excessive heel whip, be sure to take a video recording or several pictures from behind.
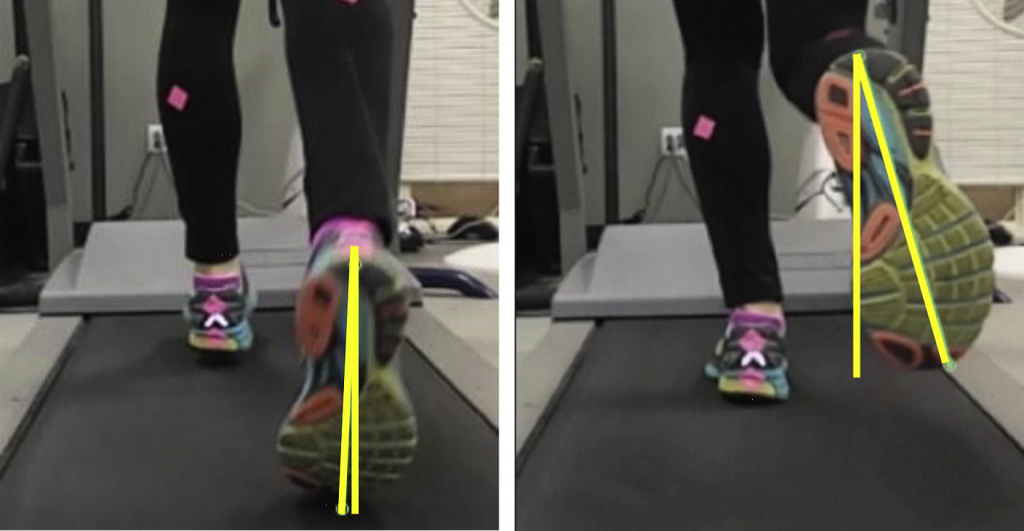
The picture below is taken from an article by Richard Souza et.al. (2015) and show as the right foot comes off the ground, the heel rotates medially (towards the midline of the body), and the toe rotates laterally (away from the midline of the body). This movement is named according to the direction the heel moves relative to the midline of the body, or medial heel whip. Other investigators use the term “adductory twist” (Keven Kirby DPM 2009). Dr. Kirby has an excellent video demonstrating adductory twist on his YouTube channel.
For some individuals, the heel whip occurs in the opposite direction. The heel moves away from the midline of the body and the toe moves toward the midline of the body. This is called “lateral heel whip” or “abductory twist”.
In my experience, when I ask patients how they feel about their running form, they often say, “I have been told I have a kick out” on one side. This could be an asymmetrical excessive heel whip.
A heel whip is a normal movement that occurs in all runners. Dr. Souza did an interesting study of 256 recreational runners (both non-injured and injured runners) and determined more than half had heel whip greater than 5°. There were also twice as many medial heel whips compared to lateral heel whips and the magnitude and/or speed of heel whip between the right side and left side can be different.
Gait analysis traditionally focuses on the stance phase, when the foot is on the ground. Stance phase is when forces are much larger in comparison to the forces occurring during swing phase, when the foot is off the ground. Heel whip occurs at the transition from stance phase to swing phase. It is likely the root cause of the heel whip is related to forces developed during stance phase and the excessive movement is occurring because of the recoil or elastic stored energy that happens because of the friction between the bottom of the foot and the ground.
The mechanics of heel whip is complex and multi-faceted. A ground foot connection that has greater friction also has a greater likelihood of being mismatched in clockwise and counterclockwise movements and forces that are occurring in the lower extremity, pelvis, trunk, and arms. One factor affecting the magnitude and/or velocity of the heel whip is the amount of friction between the bottom of the foot and the ground - greater friction will lead to larger and/or faster heel whip. Cleats, waffle soles or shoes with good traction increase the amount of friction. Barefoot or skin has more friction than some shoes. Surfaces which have less friction such as carpet, pea gravel, clay tennis courts, and wet grass are going to have less friction than the treadmill belt, cement, or asphalt surfaces.
Heel Whip and Injury
It has not been determined if large and/or fast heel whip is predictive or associated with running injuries. Dr. Clare Milner of Drexel University has measured the twisting force (free movement on transverse plane) associated with heel whip during stance phase when running, and was able to predict 66% of the cases of tibia stress fracture in runners.
It has been my experience injured runners with a larger amount of and/or rapid heel whip on the injured side of the body report injuries such as plantar heel pain, medial tibia stress syndrome, tibia stress fractures, patella femoral arthralgia, iliotibial band syndrome, and hip tendinopathy.
If the magnitude of the heel whip is asymmetrical, showing larger and/or rapid heel whip on the injured side compared to the non-injured side, this relationship deserves deeper investigation. Until more research and evidence becomes available showing a relationship between large/fast heel whip and injury, my recommendation is:
If you see this:
Asymmetrical large and/or fast heel whip and there is a repetitive use injury on one side
- Asymmetrical shoe wear on the sole of the shoes underneath the ball of the feet
- Asymmetrical shoe wear in the area of the forefoot suggesting the forefoot issliding off the bed of the shoe
- Consistent asymmetrical arm swing, trunk/pelvic rotation
Don’t do this:
- Run barefoot
- Use shoes that have good traction or cleats
- Choose to run on surfaces with good traction or high levels of friction betweenthe bottom of the foot and the ground, e.g. treadmill belts and cement.
- Habitually sit with asymmetrical posture crossing knees or side saddle sitting
Do this:
- Ask a physical therapist to perform an examination to look for asymmetrical alignment of bones or asymmetrical movement such as: residual asymmetrical clubfoot, asymmetrical range of motion of tibia rotation (medial and lateral), hip rotation (medial and lateral), and spinal pelvic rotation related to scoliosis.
- Ask a physical therapist to assess the stiffness of the anterior portion of the Iliotibial band (TFL) versus posterior portion (superficial gluteus maximus) of the iliotibial band. If there is asymmetrical stiffness of the iliotibial band this needs to be addressed with appropriate intervention.
- Select shoes in which the soles have less traction or friction.
- Choose to run on surfaces which have less traction or friction (gravel trails, wetgrass, and artificial turf).
- Ask if there is conscious modification or cueing to decrease the magnitudeand/or speed of the heel whip. Unfortunately, at this time, I am not yet aware of gait retraining cues that might alter large and/or fast heel whip.
Damien Howell Physical Therapy – 804-647-9499 – Fax: 866-879-8591 At-Home, At Office, At Fitness Facility – I come to you, I do home visits Damien@damienhowellpt.com