Osteoarthritis – Bad News More Than Good News
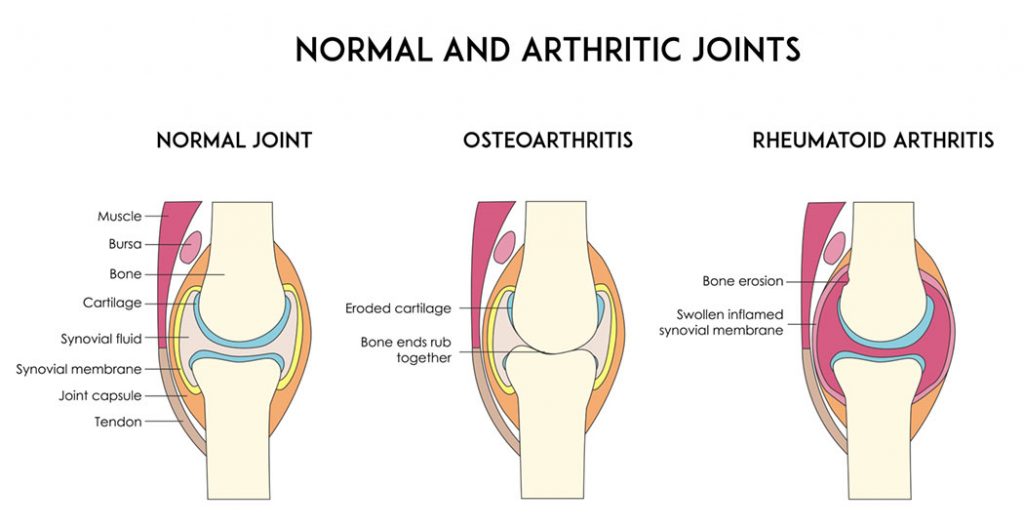
Osteoarthritis occurs in a joint when there is more degeneration of the joint cartilage than regeneration of the joint cartilage. Cartilage is a soft tissue on the ends of bones. Cartilage provides a smooth surface to allow free movement of joint, provides a cushioning, and for joint stability. Cartilage tissue is poorly designed for repair and regeneration. Cartilage does not have blood supply to facilitate healing. Cartilage does not have nerves, so we are in the dark when the cartilage tissue is being damaged. Cartilage can become frayed, cracked, and degenerates. Eventually it can worsen and effectively the cartilage fails and then ends of the bones rub and bang on each other. Bones have nerves and this is when the joints become painful. The joint failure is a very slow process.
We do know the risk factors for developing joint failure (osteoarthritis) are many including: which parents you choose (genetics); obesity; hormonal imbalances; excessive joint loading; and prior joint injury/surgery.
Osteoarthritis can occur without a history of joint injury. However an injury to the joint ligaments, and/or injury to the joint cartilage guarantee the joint will develop osteoarthritis at a later time. This is called post traumatic osteoarthritis. The only question is will it take 10 years or 40 years after a joint injury for the symptoms of osteoarthritis to develop. Significant injury to joint ligament and capsule results in a 10 fold increase risk of developing osteoarthritis at a later time. Significant injury to the joint cartilage results in a 20 fold increase risk of developing osteoarthritis at a later time. A young athlete with joint injury is at high risk for developing post traumatic osteoarthritis before age of 40. This can lead to individual having post traumatic osteoarthritis for more than half their life.
The bad news
There is no cure for osteoarthritis. The common interventions such as: glucosamine supplements, opioids; over the counter pain medications, non-steroidal anti-inflammatory medication; viscoelastic joint injections; steroid joint injections; arthroscopic surgery; fish oil, homeopathic remedies; and other stuff have no or limited symptomatic benefit. Joint reconstructive surgery used for injured joints essentially is a controlled joint trauma effectively increasing risk of developing post traumatic osteoarthritis later in life. Fortunately, most of these interventions do no harm but the bad news is these interventions are not effective or of limited effectiveness.
Currently there is no disease modifying drugs available for osteoarthritis. There are disease modifying drugs available to slow the progression or lead to remission of rheumatoid arthritis and multiple sclerosis. There is no vaccine for osteoarthritis
“None loves the messenger who brings bad news” Sophoclis Antigone
The good news:
One of the risk factors for osteoarthritis that we do have control over is body weight. Excess body weight has direct effect on osteoarthritis. Individuals who are overweight (Body Mass Index of 25 to 29) are 2.5 times more likely to develop knee osteoarthritis and those who were obese (body mass index of >30) are 4.6 times more likely to develop osteoarthritis. Body Mass Index calculators are available on the internet; just enter your height and weight.
Different research groups have shown a positive effect on improving symptoms associated with osteoarthritis by decreasing body weight. Research has shown that >5% reduction in body weight will result in moderate to large improvements in self-reported disability. Losing >10% of body weight resulted in 40% reduction in pain. Individuals who are more disabled before losing weight need to achieve a 10% reduction in body weight in order to appreciate an improvement in symptoms. Whereas, individuals who are less disabled before beginning weight loss they can achieve appreciable reduction in symptoms with less reduction in body weight.
Sadly, research has shown healthcare professionals frequently do not counsel patients with osteoarthritis regarding weight management interventions. You may need to be assertive and request information.
One of the functions of joint cartilage is to act as a shock absorber. Decreasing body weight decreases the repetitive loading or shock to joint cartilage. Interestingly, research has shown individuals who are obese are at increased risk of developing osteoarthritis in the hands and fingers. This increased risk appears to be separate from the mechanical effect of increased loads on joint and there may be a metabolic link between fat tissue and degradation of joint cartilage.
For large joints such as knee, hip, and shoulder surgical interventions which replace injured joint cartilage (joint replacement) is a viable option for management of osteoarthritis. Unfortunately it is not a great option. Research shows 1 in 4 patients undergoing joint replacement surgery are not satisfied with the outcome. Currently the spine joints are not replaceable. The success for replacing small joint fingers, ankles, toes the success is less positive.
The bottom line:
- Avoid joint injury, strategies and tactics to prevent joint injury are important
- Whether you have history of joint injury or not avoid becoming overweight/obese
- If you are overweight, weight loss should be a priority both before and after joint replacement surgery
- If you are overweight suffering with osteoarthritis work with a Physical Therapist to develop a plan of care to safely exercise and reduce caloric intake to decrease weight to decrease impact loading on joints and joint pain.
Damien Howell Physical Therapy – 804-647-9499 – Fax: 866-879-8591
At-Home, At Office, At Fitness Facility I come to you, I do home visits
Damien@damienhowellpt.com