When Tendons Turn to Fat: Lessons in Clinical Uncertainty
Dunning-Kruger effect - I know everything:
For years, I explained to my patients the benefit of strengthening exercises in degenerative tendinopathy in a simple way:
- A tendon contains many fibers. If some are damaged or torn, strengthening may improve the capacity of the remaining healthy muscle-tendon units to compensate.
- Over time, the damaged fibers may heal with scar tissue or fibrosis.
- Exercise may then help shape and align that disorganized scar tissue.
I know this because it makes sense, and it fits the way I see the problem. Of course, this unquestioning way of knowing is naive and dangerous.
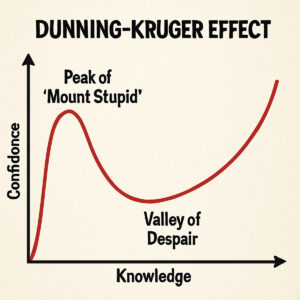
There is more to this than I thought:
A 70-year-old male with a 4-month history of shoulder pain related to swimming, I will call him Sam Swimmer, with a clinical diagnosis of rotator cuff tendinopathy. The MRI showed a partial-thickness tear of the supraspinatus and long head of the biceps tendons. In addition, there was a small amount of fatty infiltration of the supraspinatus tendon.
As an experienced Physical Therapist, this finding of fatty infiltration of the muscle-tendon unit was a pathology that I was unfamiliar with. And it stimulated many questions.
What is fatty infiltration of a muscle tendon unit?
Fatty infiltration of a muscle-tendon unit is a degenerative medical (chronically damaged, as in tendinopathy or tears) condition where normal, healthy tendon-muscle fibers are progressively replaced by fat cells (adipocytes) instead of healthy tendon cells or muscle fibers. Think of it like the marbling of a beef steak, except it is a human muscle tendon. It significantly degrades the strength, elasticity, and function of the muscle tendon unit. (Osti et al., 2013)
Fatty infiltration of the human muscle-tendon unit is analogous to marbling of fat that occurs in beef
It frequently occurs in the shoulder and hip region, but can occur in other muscle tendon units. (Kajdi et al., 2025; Lee et al., 2024)
I am never going to understand this:
The exact mechanism or pathophysiology explaining it is uncertain.
One theory is that there is increased space between tendon cells and tendon fibers after injury. The space can be full thickness of the tendon (tendon tear/rupture) or partial tendon thickness. This leads to mechanical unloading of the muscle tendon unit, allowing for fat cells and fibrous tissue to infiltrate between the remaining cells and fibers.
Now I know the natural progression of damaged tendon fibers does not always result in fibrosis or scarring but may result in fatty tissue infiltration.
Is fatty infiltration of the muscle-tendon unit reversible?
There is very little research directed at the question of reversibility of fatty infiltration of the muscle-tendon unit, but it is largely considered irreversible using current surgical and Physical Therapies.(Bowen et al., 2025), (Osti et al., 2013)
It is starting to make sense:
Prevention and early identification
If fatty infiltration of the muscle-tendon unit is irreversible—or difficult to reverse—then prevention becomes especially important. Early identification may also matter, recognizing a small amount of fatty infiltration may improve the chances of limiting progression and preserving function.
Risk factors associated with the development of fatty infiltration in a muscle-tendon unit include:
- Size of tears.
- Too many birthdays
- Female sex
- Obesity
- Full-thickness tendon tears
- Longer symptom duration
- Statin use. (Yamakado, 2024)
- Extra-articular steroid injection. (Lee et al., 2024)
Identifying early muscle-tendon fatty infiltration requires diagnostic imaging, such as MRI or diagnostic ultrasound. (Nasr et al., 2023)
Physical Therapists are often the first healthcare professionals to diagnose tendinopathies. Unfortunately, most Physical Therapists’ ability to order diagnostic imaging is limited because of statutory barriers. (Davis et al., 2022)
As a Physical Therapist, I now see the value of considering early fatty infiltration as part of the differential diagnosis in tendinopathy. When it is suspected, requesting consultation for appropriate diagnostic imaging can help guide the differential diagnosis process and plan of care.
Trust me, it’s complicated:
Strengthening exercises are the cornerstone of management of tendinopathy; the most effective type of strengthening exercise, concentric, eccentric, or isometric, remains debatable.
Is there a way to design strengthening exercises so that, at the tissue level, optimal loading of the damaged or torn tendon fibers can potentially prevent the development of fatty infiltration?
The work of Keith Baar and colleagues at UC Davis, based largely on animal models, suggests that mechanical loading can be designed at the tissue level to bypass the natural stress-shielding that occurs in partial-thickness tendon injuries. Their research also indicates that stress relaxation may help deliver more appropriate loading to healing fibrotic tissue. (Tam & Baar, 2025)
Stress shielding in partial-thickness tendon injuries
Stress shielding occurs when a specific region of a tendon is protected from normal physiological stress, including the mechanical loads and tension needed for tissue adaptation.
Stress shielding can have beneficial effects when the uninjured tendon fibers temporarily shield the injured fibers from excessive load, reducing the risk of further damage.
Stress shielding can also become a problem if the injured fibers remain underloaded. Without enough mechanical stimulus, the healing tendon may not be remodeled effectively. In that situation, prolonged underloading may contribute to maladaptive tissue remodeling and could be one factor associated with fatty infiltration.
Stress relaxation in partial-thickness tendon injuries
Stress relaxation is using prolonged static loads, such as isometric contraction of the muscle-tendon unit, temporarily relaxing the strong fibers, allowing the injured healing fibers to experience a therapeutic loading stimulus. In effect, bypassing the stress shielding.
Imagine a “Chinese Finger Trap” with a few fibers that have tears. Pulling away tightens the grip, mimicking stress shielding. While pushing inward, loosen the braids mimicking stress relaxation. The hypothesis is holding static load is held for a long duration, 30 to 45 seconds, creep and relaxation of the uninjured fibers occur. Then, therapeutic loading of the injured fibers can occur – stress relaxation.

Case Example:
What I am currently experimenting with clinically is using isometric exercise. The approach builds on concepts others have described for Achilles and patellar tendinopathy.
I am thinking of using isometric exercise to load the injured tendon, reduce stress shielding, promote stress relaxation, and possibly limit fatty infiltration. The following is my recipe for using isometric strengthening.
- Choose a joint position that isolates the involved tendon and limits neighboring joint contribution.
- Choose the position on the muscle-tendon length. Patients should consult a Physical Therapist; Physical Therapists may use Kendall’s “active insufficiency” concept. (Kendall)
- Progress positions from the shortest length to mid-range, to the “sticking” or painful point, and finally to a lengthened or compressive position of the muscle-tendon unit.
- Ramp effort slowly—no jerking—and keep pain mild, no more than 3 out of 10.
- Use the highest tolerable effort for 30 to 45 seconds per set.
- Alternate shorter daily sessions of 5 to 10 minutes with longer daily sessions of 15 to 20 minutes.
- Progress effort and hold duration gradually over days or weeks as symptoms allow.
- As performance improves, vary the position slightly to stimulate different tendon regions, especially in crescent-shaped shoulder and hip tendons.
What the recipe should feel like: During the exercise, monitor for signs of creep and stress relaxation, such as a gradual softening of tissue tension or small increases in range of motion. It is also common to notice fatigue, shaking, cramping, or temporary weakness during the hold. Afterward, symptoms of joint pain or discomfort may decrease. If these positive responses occur, the dosage is likely appropriate. If you do not notice any meaningful change, the exercise may be underdosed. If symptoms increase after the session, the exercise is likely to be overdosed. Adjust the position, effort, duration, or frequency the next time. Apply the Goldilocks Zone.
Unanswered Questions
Person-level outcome
Over 14 weeks, Sam Swimmer reported significant improvement after using the isometric exercise recipe described above. (Docking & Cook, 2019)
Tissue-level uncertainty
However, no repeat MRI is available, so it is not possible to determine whether the recipe altered the fatty infiltration of the supraspinatus tendon.
Building better evidence
Fatty infiltration of a muscle-tendon unit is an example of constructing a logical explanation; the explanation becomes accepted as truth, and new evidence reveals the original explanation was incomplete.
When fatty infiltration of a muscle-tendon unit is suspected, diagnostic imaging before and after intervention may help clinicians track tissue-level change over time.
For Physical Therapists, this kind of imaging-informed follow-up could help gather evidence to support—or challenge—the current assumption that fatty infiltration is irreversible. (Bogdanov et al., 2021)
References:
Bowen, E., Waque, A., Su, F., Davies, M., Ode, G., Lansdown, D., Feeley, B., & Bedi, A. (2025). Muscle Health & Fatty Infiltration with Advanced Rotator Cuff Pathology. Curr Rev Musculoskelet Med, 18(4), 160–172. https://doi.org/10.1007/s12178-025-09955-w
Davis, D. L., Almardawi, R., Awan, O. A., Lo, L. Y., Ahmed, S. R., Jubouri, S., & Gullapalli, R. P. (2022). Supraspinatus fatty infiltration on MRI among older adults receiving physical therapy as initial management for clinically suspected rotator cuff tear: A pilot study. J Clin Imaging Sci, 12, 66. https://doi.org/10.25259/JCIS_138_2022
Kajdi, G. W., Goller, S. S., Zingg, P. O., & Sutter, R. (2025). Fatty infiltration of the gluteus medius and minimus muscles: volumetric analysis of both hips in patients with unilateral greater trochanteric pain syndrome using 2-point-Dixon MRI. Insights Imaging, 16(1), 282. https://doi.org/10.1186/s13244-025-02175-3
Lee, J., Lho, T., Lee, J., Lee, J., & Chung, S. W. (2024). Influence of Frequent Corticosteroid Local Injections on the Expression of Genes and Proteins Related to Fatty Infiltration, Muscle Atrophy, Inflammation, and Fibrosis in Patients With Chronic Rotator Cuff Tears: A Pilot Study. Orthop J Sports Med, 12(6), 23259671241252421. https://doi.org/10.1177/23259671241252421
Nasr, A. J., Pierson, C. J., Tzen, Y. T., Khazzam, M., Jain, N. B., & Lin, Y. S. (2023). Emerging Role of Quantitative Ultrasound-Based Imaging Techniques for Characterizing Rotator Cuff Tears: A Scoping Review. Diagnostics (Basel), 13(12). https://doi.org/10.3390/diagnostics13122011
Osti, L., Buda, M., & Del Buono, A. (2013). Fatty infiltration of the shoulder: diagnosis and reversibility. Muscles Ligaments Tendons J, 3(4), 351–354.
Tam, K. T., & Baar, K. (2025). Using load to improve tendon/ligament tissue engineering and develop novel treatments for tendinopathy. Matrix Biol, 135, 39–54. https://doi.org/10.1016/j.matbio.2024.12.001
Yamakado, K. (2024). Influence of statin use on progression of postoperative fatty infiltration in the arthroscopic rotator cuff repair. Eur J Orthop Surg Traumatol, 34(8), 3955–3960. https://doi.org/10.1007/s00590-024-04084-5
The information on this website is not intended or implied to be a substitute for professional medical advice, diagnosis, or treatment. You are encouraged to perform additional research regarding any information available through this website, with other sources, and consult with your physician