Total Knee Joint Replacement – Are You Satisfied? Gait Analysis & Training Can Provide Post-Op Improvements
Pain and stiffness associated with osteoarthritis in knee joints can result in a limp, gait deviations and gait compensations.
Gait deviations are variations from what is perceived as normal walking or running. These deviations are described as limitations, restrictions or weaknesses that lead to lack of mobility, stability or symmetry of movement.
Gait deviations also may create pain or may be a subconscious result of avoiding pain. Gait deviations are synonymous with gait compensations, which can be a good thing or a bad thing.
The two factors shape automatic or subconscious gait compensations. Instinctive compensation is to move in a way that avoids pain or to move in a way that takes the least amount of energy.
Gait Deviations Associated With Knee Osteoarthritis
Common gait deviations associated with pain and stiffness of knee-joint osteoarthritis include:
- Slow velocity
- Listing or leaning of the trunk to the side (lurching)
- Excessive pelvic drop (hippy-dippy gait)
- Lateral or medical deviation or thrust of knee (shimmy)
- Insufficient knee extension or walking with bent knee
- Insufficient knee flexion (straightening) during swing phase of gait
- Excessive out-toeing during stance phase of gait when foot is on the ground
Gait Deviations After Total Knee Replacement
Studies have shown that many of these gait deviations continue even after the impaired knee joints have been surgically replaced. After total knee replacement surgery, patients report less pain. But they often continue to ambulate, or walk, with measurable gait deviations.
Arguably the reason for ongoing gait deviation is that is has become a bad habit. Months of ambulating with a limp to avoid pain becomes the new normal. Gait compensation continues despite the fact that the impairment has been resolved.
Strengthening exercises alone are not enough to fix gait deviations. A better and more thorough approach is to include gait training coaching and cueing to alter observed gait deviations.
After knee replacement, each of the noted gait deviations should no longer be needed because joint pain has been eliminated. Continuing to walk with a gait deviation may lead to development of another pain problem, such as heel pain, hip pain or back pain – a whack-a-mole effect!
If you have had a total knee joint replacement surgery self-assessment -- or if your spouse complains that you still walk with a limp -- request additional assistance from your physical therapist on gait training guidance.
Gait analysis and gait training can be used to address each of the above-mentioned gait deviations.
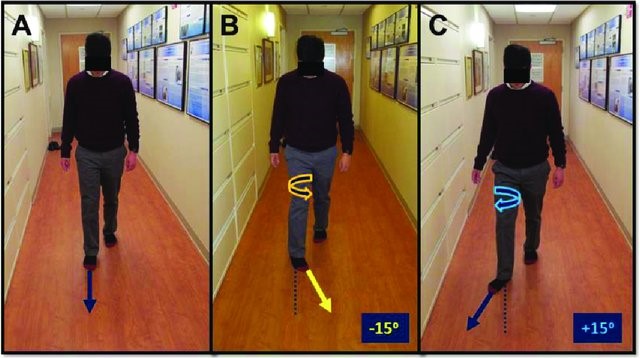
Excessive Out-Toe Gait
Gait training for a gait deviation of excessive out-toeing can help achieve a higher level of function and satisfaction after knee replacement surgery.
“Toe out” is the degree to which the foot is oriented outward, away from the midline of the body, with respect to the direction of forward progression. Out-toeing greater than 15 degrees from the line of forward progression is considered deviant (see illustration C below). Out-toeing more than 5 degrees greater than the uninvolved side is considered deviant.

If you have had a knee replacement, consciously decreasing the degree of toe-out can eliminate your gait deviation without increasing pain.
But if a conscious effort to decrease the degree of toe-out increases your knee pain, it is likely the thigh muscle is not strong enough to allow walking with appropriate alignment. This can be addressed with additional strengthening exercises for the thigh muscles. One also could argue that a conscious effort to walk with less than 15 degrees of toe-out could be a way to progressively strengthen the weak thigh muscle.
If you came into the world with more than 15 degrees of toe-out, your bony structure is deviant from the norm. A physical therapist can assess to determine whether the toe-out deviation is a result of a bony structural variation. In this case walking with toe out should be allowed or encouraged.
The verbal cue to alter the gait deviation can be as simple as, “Don’t toe-out so much” or “Push your heel out to the side when walking.” A better cue is to provide external feedback of the movement and alignment of the leg.
A mirror in front of a treadmill is one way to provide external feedback.

Using painter’s tape on the ground as a reference point to the line of progression also can provide external feedback. Notice the green tape on the mirror in the picture above providing a target for right-foot alignment.
Walking through a mud puddle or in sand and turning around to see the alignment of the foot relative to the line of progression is yet another way to provide external feedback.

Are Your Surgery Results What You Expected?
If you are not satisfied with the results of your total knee joint replacement surgery, be more assertive. Ask for a second opinion regarding the post-operative rehab program.
The investment of time and resources made in joint replacement surgery requires an investment of sweat equity in your post-op rehabilitation program.

A on demand-video webinar exploring this topic is available at Plus by Physiopedia entitled “Back & upper leg regional pain & gait deviations”
Use this code – “Damien25” for a 30% discount to access this webinar as well as the more than 500 continuing education webinar courses available at Plus by Physiopedia. This is the link http://bit.ly/DAMIEN25 with the 30% discount code embedded
Damien Howell Physical Therapy – 804-647-9499 – Fax: 866-879-8591 At-Home, At Office, At Fitness Facility – I come to you, I do home visits Damien@damienhowellpt.com